Parathyroid Surgery
Introduction
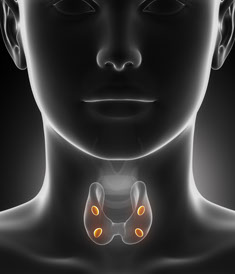
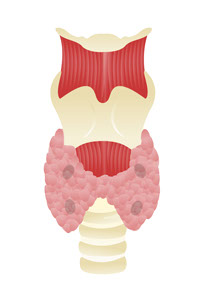
The parathyroid glands are four (or more) small glands that sit on either side of the thyroid gland in the neck. They are part of the endocrine system, and control calcium levels in the blood by releasing a hormone called parathyroid hormone (PTH). Calcium is an important element required for the function of the nervous system (including the brain), muscles and bones. As the blood filters through the parathyroid glands, they detect the amount of calcium present in the blood and respond by making more or less parathyroid hormone (PTH). When the calcium level in the blood is too low, the cells of the parathyroid glands sense it and make more parathyroid hormone. Once the parathyroid hormone is released into the blood, it circulates to act in a number of places to increase the amount of calcium in the blood (by removing calcium from bones, and increasing calcium absorption from the intestine and kidneys). When the calcium level in the blood is too high, the cells of the parathyroid glands make less parathyroid hormone (or stop making it altogether), thereby allowing calcium levels to decrease.
Hyperparathyroidism
In most patients with hyperparathyroidism, one (or more) of the parathyroid glands behaves inappropriately by constantly making excess parathyroid hormone regardless of the level of calcium. This leads to excessively high levels of calcium. The most common cause of excess hormone production (hyperparathyroidism) is the development of a benign tumor in one of the parathyroid glands, which is called a parathyroid adenoma. This accounts for 95% of all patients with hyperparathyroidism. Other causes include hyperplasia (enlargement) of all four glands, or very rarely, a cancerous parathyroid gland.
Nearly all patients with hyperparathyroidism will have some symptoms. Easily identifiable symptoms include kidney stones, bone pains, heart palpitations (arrhythmias), and depression. Some patients present with symptoms, which are less obvious, such as high blood pressure, the inability to concentrate, irritability, forgetfulness, loss of energy and fatigue, frequent headaches, dizziness and gastro-esophageal reflux. Nearly all patients report a significant improvement in their symptoms after surgery. Studies also indicate that patients with untreated hyperparathyroidism are at a greater risk for cardiac disease and early mortality.
Diagnosis
Hyperparathyroidism is diagnosed by detecting elevated Calcium and normal-high Parathyroid Hormone (PTH) levels in the blood. As mentioned earlier, up to 95% of cases of hyperparathyroidism are due to the presence of a benign tumor in one of the parathyroid glands (parathyroid adenoma). The adenoma may be localized preoperatively using the following imaging studies:
- Sestamibi scan: This is a specialized scan done in a nuclear medicine facility. Sestamibi is a small protein, which is labeled with the radiopharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with hyperparathyroidism, and is absorbed readily by the overactive parathyroid gland. This gland alone will absorb the radioactive tracer and “light up” on the scan, allowing identification of the adenoma among the four glands.
- Ultrasound: This imaging modality uses sound waves to detect masses in the neck, and does not require the use of contrast material or radioactivity. This technique is often used to identify abnormalities in the thyroid gland and can be very useful to differentiate parathyroid growths from the thyroid gland itself.
Parathyroid Surgery
The large majority of patients with hyperparathyroidism will have this disorder due to an adenoma. Removal of the adenoma is a quick and effective treatment for hyperparathyroidism. You do not need all your parathyroid glands, and once the overactive adenoma is removed, the remaining glands will take over to keep your blood levels of calcium normal.
The surgery is performed in the hospital under general anesthesia. Patients may spend a night in the hospital after the surgery. Preoperative imaging studies (Sestamibi scan and/or Ultrasound) will often localize the adenoma. This allows for a minimally invasive approach using a small incision to help identify and remove the adenoma. An intra-operative blood draw to check the Parathyroid hormone (PTH) level after the adenoma has been removed can also help confirm removal of the offending gland. Parathyroid hormone has a very short half-life (~2 minutes), which means that when the overactive gland has been removed, the high levels of PTH that have been secreted by this gland disappear from the blood at a rapid pace. The essence of the surgery is to remove the offending gland while leaving the other structures of the neck intact. Important structures in the area of the parathyroid glands include the thyroid gland, trachea (windpipe), esophagus, and recurrent laryngeal nerve (which allows you to move your vocal cords).